


By far and away the most common expression of anguish I hear from workers who are prescribed medicinal cannabis products is a fear that, if workplace and roadside drug testing laws doesn’t hurriedly adapt, they will be back on a Selective Serotonin Reuptake Inhibitor (SSRI) for life.
The thought fills some of them with terror. Many people meet the news with a resigned, grim determination that they can see it through for another couple years until the laws change. They’ve found a better way to treat DSM Diagnosis X with cannabinoids and it’s a unique form of torture to have to go back onto the prior meds which mostly slapped away at the problem but with harsh and intolerable side effects. Withdrawing from these drugs and the seeming impossibility for many people to do so without considerable disruption to a regular working life all changed with the Pandemic and Lockdowns and the mainstream media is finally catching up.
After 36 years of use and on balance, SSRIs may have been a temporary lifesaver for some, BUT they have been a pharmacological dead-end for most and a downright danger for a minority of patients. SSRIs never lived up to their marketing hype and they harmed people. It’s that simple.
Tomorrow night, Four Corners will air the long-awaited BBC Panorama investigation, ‘The Antidepressant Story’. Long-awaited by those who have been patiently waiting twenty years for the inevitable legal shitstorm to flow from the long term use of SSRIs. Those who have read Harvard academic psychiatrist Dr Joseph Glenmullen and follow anything that journalist Robert Whitaker/Mad in America publishes and also believe that Medical Anthropologist and Psychologist Dr James Davies’ Sedated: How Modern Capitalism Created our Mental Health Crisis is, outside of climate change literature, the most important non-fiction book of the 21st century thus far.

If you are ambivalent to them or amongst the third of folks who claim a benefit from SSRIs, great. One thing you appreciate in the medicinal cannabis law caper is no-one ought be attaching stigma to whatever gets someone else through the night. No pill shaming here. I encourage you to watch Four Corners/Panorama then read Melbourne/NT Psychiatrist Dr Sam Lieblich’s searing piece in Overland from three years ago.
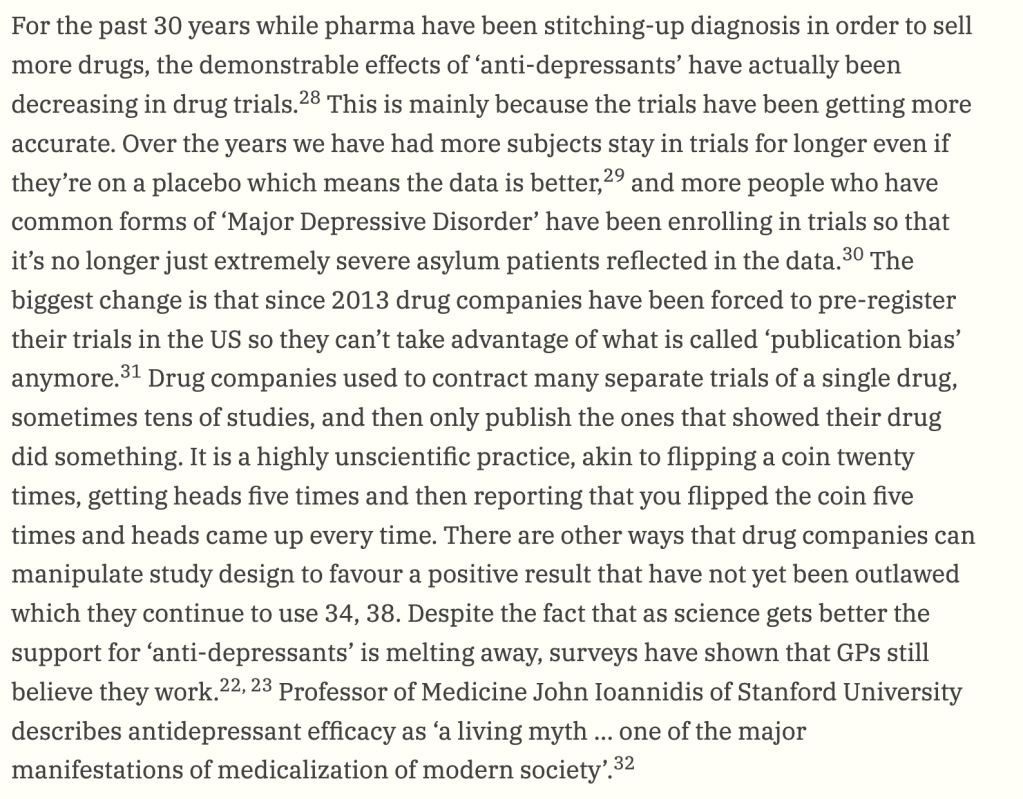
If you’re no stranger to the unique hell of the devil trying to pull your brain out through your kneecaps that is SSRI withdrawal, you’ll no doubt tune in and don’t need chapter and verse on the history of this class of medicines. For the newbies, go watch Dopesick and Painkiller. The same marketing tools and techniques used to market opioids were utilised with SSRIs. The same marketing techniques were originally pioneered by the Sackler family with, another antidepressant-type creature, Valium. The playbook never changed from the 1950’s to the early 2000’s. Doctors just became less curious and more prone to accept whatever a dollybird/ken-doll sales rep told them. Millions spent in the shameless bribery of doctors with weekends away, shmick dinners and shiny pens buried the harms and obscured scientifically verifiable facts behind a methodology that conflated the statistically significant with the clinically insignificant and vice versa.
SSRIs came into being as a result of a late 80’s patent rush and guys in white coats flinging patentable molecules at histamine receptors. Our knowledge of histamines ultimately stems from powdered European aristocrats huffing ether and other whacky gasses in the 1700’s, getting munted then bumping into sharp table corners and realising they felt no pain. Not the most auspicious of beginnings for a line of science that eventually gave us anaesthesiology, a branch of medicine for which we’re all eternally grateful.
But in the realm of treating the creations of the DSM (depression /anxiety/PTSD/trauma), we’ve got an armada of emerging options from cannabinoids through to psychedelics showing remarkable promise in treating those conditions. More promise than anything patented by the SSRI Club over the last 30 years, anyway. If you’re reading this far then I’m preaching to the choir. You all know the drill and the disclaimer speel that has to come next.
There is not enough evidence to the Phase III triple blind standard for anyone to make a statement any stronger than “showing promise” when it comes to medicinal cannabis products approved under SAS B or prescribed by APs.
On Four Corners/Panorama you’ll see the methods imposed by the SSRI patent sponsors to get these drugs over the line. Those patents are mostly since expired but liability will ultimately lie with the companies who sponsored the products through FDA/MHRA/TGA approval by funding the studies to the Phase III triple blind standard for what makes a product both efficacious and safe. If you’ve been wounded by an SSRI or lost years of your life in what David Heilpern calls the Barely Bearable Blur, you’ll be pissed off. And you will want to talk to lawyers about it. If you lost loved ones to the throes of a poorly planned or monitored “SSRI Switcheroo”, you’ll be absolutely filthy how trial data was interpreted and …well, just watch the show tomorrow night and make up your own minds.
SSRI litigation is in its infancy but it has been a thing for roughly ten years now (in the US) with a handful of cases here. But that’s a discussion for an audience that has actually watched the thing. I’ve resisted temptation to sus out a version of it which skirts IP rights as between our Anglophone Aunties (BBC and ABC). I’m hoping that the Panorama story addresses litigation.
Those of us in attendance at the Sunday morning session at the UIC Symposium featuring Dr James Stewart won’t soon forget it. We’re seeing the same things, professionally. Workers/patients who have struggled for years to withdraw from a prescribed drug that was harming them (or barely helping them enough to warrant endurance of the side effects) who find tremendous success on cannabinoids but then hit life speed bumps like retaining a driver’s license or holding down a job. Going back on SSRIs is simply not an option for many people, even it means holding down a job or a driver’s license.
On the balance of probabilities, harm is certainly foreseeable for those with an already documented medical history of struggles with SSRI withdrawals. Reasonably foreseeable harms are the harms we’re all meant to avoid (and to document our notice and steps taken to mitigate). On this analysis, step one should always be to prioritise a continuance of existing CBD:THC regimes if a Dr has good records of patient progress and correct titration. How to square this obligation to a patient with the layer of medico-legal obligations that presently compel a medical practitioner to form the professional opinion that SSRIs are safe long term?
After watching Four Corners/Panorama – am keen to know how many medical insurers would feel comfortable with the status quo, knowing that none of these sedation biscuits have got ANY reliable safety data beyond that of a few months/years (interested to see which number the BBC goes with). Plus the empirical evidence of harm is mounting. 1980s/90s/00’s-Sales rep lines and marketing materials that claimed no harmful withdrawals or potential of addiction with SSRIs and that they are safe to take for life are starting to look pretty shady now. The lawyers, Sith Boffins and marketers who colluded to shepherd the whole shebang through drug approval processes acted unconscionably. Same as they did with opioids and benzos before that.
Yet an Australian doctor having a conversation with another professional on a podcast about transitioning from SSRIs onto CBD:THC (and increasingly, minor cannabinoids) would need to exercise caution in ensuring the published conversation was balanced on the pros and cons of use of cannabinoids in SSRI withdrawals and was scientifically & factually sound and didn’t promote the use of schedule 4 or 8 cannabis medicines. That’s the frustration. SSRI sponsors lied and manipulated data. People were (and continue to be) harmed. Medical practitioners championing naturally occurring alternatives risk heavy fines for promoting any success stories of people who have safely transitioned off SSRIs onto cannabinoids.
Covid Lockdowns and the Work From Home Revolution served as a catalyst to speed up the downfall of SSRIs. WFH aided many people in finally withdrawing from sedation biscuits after numerous unsuccessful attempts at doing so. Thieving some lines below from my recent Drive Change blog thing.
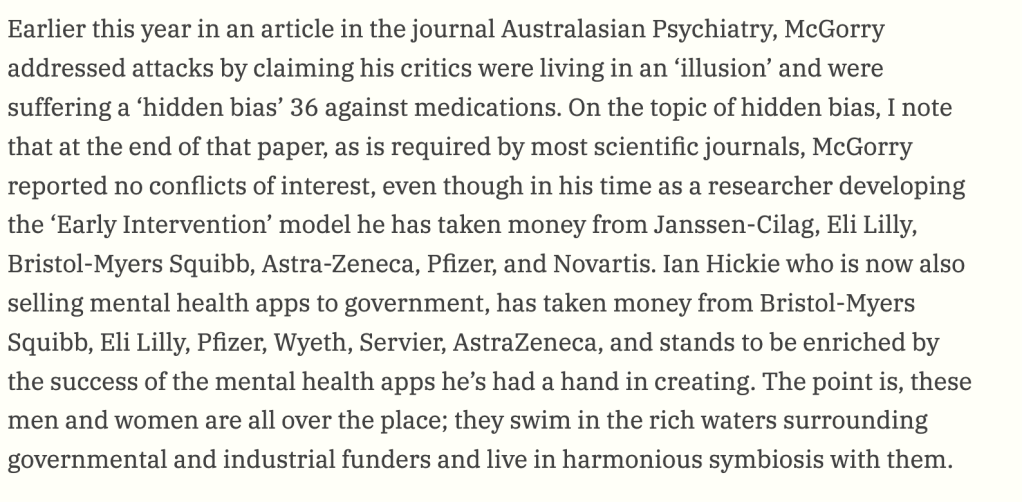
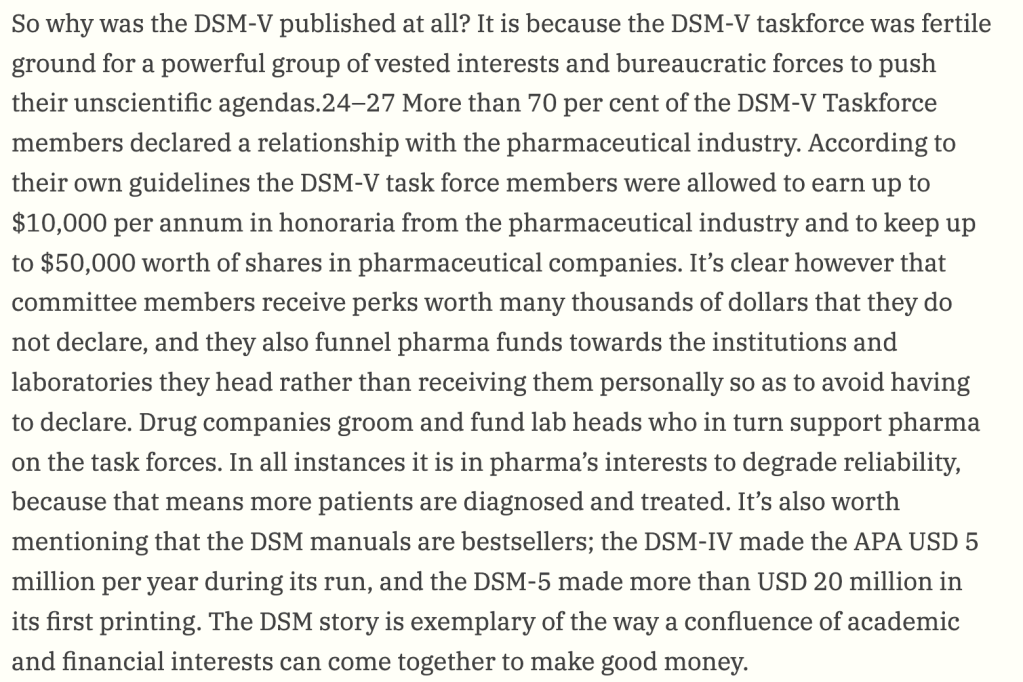
Naturally, the academic doyens of psychopharmacology who were funded off of SSRIs have been in no rush to backtrack any of their earlier, well-funded work. Go read Sam Lieblich very closely on this point. You can’t win cases if you don’t have an expert in the relevant field to back your case up. It’s all down to the DSM boyos. But boy oh golly gee – SSRIs involve the reduction in pleasure or even basic functionality of a person’s sex life, so yes – there have been some settlements. American plaintiffs in particular are very sensitive about loss of amenity in a sex life. There is nothing more frightening that the following words used in combination: Permanent Sexual Dysfunction. At-least Freud and Jung got that right.
SSRI litigation has remained in its infancy mostly because all the top scientist expert witnesses were bought out by SSRI interests a long time ago. There has, unsurprisingly been minimal effort to pause and review the standards of the science done on SSRIs in the 80/90’s. Courts desperately need modern light side of the force boffins to reset the goalposts on where harm was done based on what they have seen with their own practitioners’ and/or independently research-funded eyes, not what the literature and product sales reps told them they ought to have expected from long term use of SSRIs. The goalposts certainly need to be moved to accommodate the emerging reality that all SSRI past product sponsored research, was and is, flawed and bunk. Ambo’ Chasin’ lawyers are always going to hone in on product liability issues like this.
It is not hyperbole to state that, eventually and inevitably, many psychopharmacological research careers will be ended in ignominy and disgrace (and rightly so). Who can say how many years off it all is. There’s significant oomph to be had on reasonable reliance on the data, such as it was in the 80’s/90’s. But I’m battling to see a defence for the decades of obfuscation and denials surrounding the issue of withdrawals and PSSD.
We need a frank reassessment of what prescribers got fed by way of SSRI marketing materials. In the US, that was those horrid TV ads which are thankfully banned in Australia because all marketing of scheduled medicines to members of the public is banned. Perhaps in hindsight, if the Aussie public had seen TV ads for SSRIs they would have called bullshit much earlier on the marketing materials that were being circulated to (mostly) GP’s.
The biggest clanger to emerge in recent years being the claim from SSRI sponsors that if patients complained of withdrawal symptoms, this was in fact the symptoms of their anxiety/depression returning because of the chemical imbalance nonsense that drove the marketing of these drugs. Such marketing representations were sketchy and people have been harmed as a result. The people who colluded in the fiction need to pay up for the harms they caused.
Quoting from Leiblich below, this is one of the main reasons for the disconnect between the clinical reality that SSRIs are shithouse and unsafe compared with the official literature that courts and governments rely on which indicate the products are safe and effective. Australian Veteran campaigner Derek Pyrah and I covered this off in an early morning text exchange. Why is it so hard for the Dept of Veteran’s Affairs to grasp that when a veteran tells them that MC worked for them whilst SSRIs (and the rest of the pharma cocktail) harmed them? Governments and courts rely on the dominant position in the published and peer reviewed scientific literature. And right now, the literature reckons SSRIs are “safe and proven to be effective.”
As Dr James Stewart succinctly stated that very hungover UIC Sunday morning, “Do no harm.” Those SSRI marketing materials provided to doctors made harm happen. So who caused the harm? The product sponsors who funded the research bear a higher moral onus than the competent medical practitioner who prescribed an SSRI on the basis that the studies and safety profile vouched-for in any governmental drug approval process means that in giving Patient X, Drug Y – a prescriber consciously and genuinely believed that they were causing no harm.
It’s probably smart for all current medical practitioners in the MC bubble to keep detailed records of the progress of patients who, due to driving or workplace matters, are forced off MC and back onto SSRIs. They may not be able to consume cannabinoids until laws change, but we need some form of reliable data tracking on their welfare/quality of life since going back on the sedation biscuits. Their family/spousal views are also important. What treatment does a patient’s family think works better for them is also a valid line of inquiry worth keeping receipts for. Always keep receipts.
‘Evidence’ in a medical/scientific meaning is what sets the context and standard for a judicial interpretation of what that word means. And right now, the best evidence in a court is ultimately whatever the best evidence is in The Literature then filtered through the DSM.
‘Evidence’ causes a brainfreeze in a legal professional context when you’re hearing enough reliable and direct empirical evidence from patients (in the form of statements, affidavits etc) as to the safety and efficacy of medicinal cannabis in comparison with the neurological lucky dip that is escaping unscathed from years or decades of SSRI use.
But – Facts, Issues, Law, Conclusion – that’s the art & science of being a lawyer. That’s the job. You compile evidence, build cases and fix things in accordance with a lawyer’s paramount duty to the courts and the administration of justice.
We’ve now hit the point in Australia where medicinal cannabis law reform is butting up against the sphere of public property, involving rights to drive on public roads and (mostly) private property by way of the right to a presumption that you’re not a workplace risk as a result of the prescribed medication that you take when certain precautions are taken. This is simply a result of increased take up of MC over other medications.
We will need bravery like Dr James showed to start having honest, non-pill shamey conversations (outside the MC bubble) with people about SSRIs.
There is a lively debate at-last emerging in British / US psych fields. There’s belated recognition of the seriousness of withdrawals. The standard straw man attack line from SSRI product sponsors and their armada of well paid academics is that anyone questioning a person’s use of/perceived benefit from an SSRI is pill shaming. Key Australian academics with significant media profile and clout have deployed it here too.
If a third of people found a benefit from using an SSRI and if a third are indifferent and a third potentially harmed by these drugs, you leave be that third of people who can’t get enough of Huxley’s Soma. If it works for them and they’re happy, leave em be.
These drugs were marketed around the rubbery zinger of “the idea is the patient takes this drug for the rest of their life if they have a DSM condition.” If a person wants to do that, no-one has any right to judge, belittle, berate or boo-hoo them. And please note, a person is only a pill stooge if the commercial relationships alleged can be proven. It’s not a useful combo of words to sling around.
Again, if the Arnott’s Milk Arrowroot Biscuit of modern psychopharmacology works a treat for you and the side-effects are tolerable, then you’re one of the lucky ones where a drug developed for whatever your diagnoses may be has proven to be an effective treatment (even if the smartest psychopharmacologist or psychiatrist in the world has NO effing clue how it works. If it’s purely placebo, again, whatever gets a person through the night).
The initial SSRI patent sponsors are openly pissed at perceived cannabinoid exceptionalism in 2023 in being able to attract patients from a market that they dominate because they fucking created it. The reality is that old school pharma is secretly pissed that the natural, non-patentable world has come up with means to treat the types of illness and malaise where, “sometimes, a person is just going to need something psychopharmacological for the rest of their lives.” Cannabinoids can do it without killing a person, shortening the life of that person or shutting down the means of sexual reproduction. That last point is a kinda important thing for the survival of our species.
Right now I don’t reckon a betting person would back the original SSRIs patent sponsors to be able to eventually claim the same things. And if you are a betting person, stop gambling and mute Joel Caine.
Cannabinoids, unlike SSRIs, can achieve a therapeutic benefit without a rough-as 3-6 month upward titration and approximately same length of time for another rough ride in tapering off. SSRIs are a roll of the dice for those times in life when being temporarily numb is beneficial in coping with a temporary MH crisis. You can’t just take them for 3 months and be done with them. SSRIs involve a pharmacological intervention that, it appears, knock around the human brain in ways we’re only now properly begining to understand.
For a patient to go back to SSRIs in some cases arguably requires a person to consciously do an act that they know will harm them. That’s bonkers given what we know from [insert key highlight from Four Corners/Panorama]. Leaving square brackets in the night before it airs is intentional.
Workplace and driving laws need to accord with society’s 2023 expectation that we don’t force people back onto prescription drugs that:
- May have nixed a sex life at the garden variety level of harm; or
- May have nearly killed them at the extreme eggshell skull end of the injury and Whole Person Impairment (WPI) spectrum.
Between 1 and 2 lie a complex and heartbreaking spectrum of outcomes for people.
The balance is there to be struck so people can taper off an SSRI and take medicines containing CBD:THC without having their lives upended. Parliaments can create laws to give effect to this core principle of what we’re working towards.
We’re barely a bee stinger width into the surface of the iceberg that is long term side effects of SSRIs. This will be an additional burden on the aged care sector, which at times, may have fallen apart but for use of SSRIs (and quetiapine). SSRIs and the lives lost during a “med switcheroo” or withdrawals is likewise another iceberg and it too, is a big ‘un. Then there is the Batman Killer, James Holmes, also featured on Panorama. Families of those lost will be an important voice in the coming frank discussions that Australian society needs to have over this one basic proposition: are the pills the GP gives you for depression/anxiety just a crock of shit and are they harmful to a statistically and clinically significant number of people? If more people went on them than came off SSRIs during lockdowns, we need to have that conversation sooner rather than later.
This article is not medical or legal advice. No person should cease taking or lower their dose of an SSRI (or any prescription drug) without the supervision and advice of the person who prescribed that drug.
Whilst patentability in the cannabinoid field is lively in terms of extraction and delivery methods, there’s only so much Lockean labour than can be brought to a natural occurring thing to justify the granting of property rights in the thing. For PBR, trade marks, trade secrets/know-how and emerging areas in cannabinoid IP law, you can book a chat with me via Reparation Legal.
